Bitspec
How Medical Admissions should be designed in the age of specialized medicine
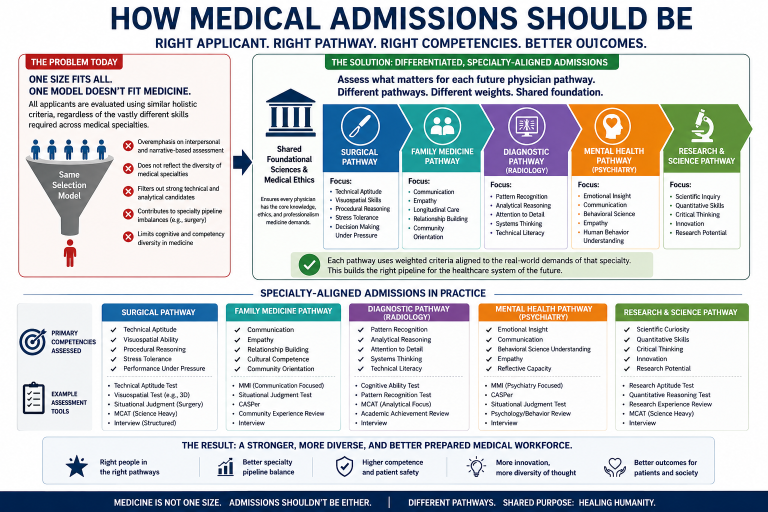
Fig. 1 Admission Policies
How Medical Admissions should be designed in the age of specialized medicine
Modern medicine is no longer a single profession operating under a single competency model.
A neurosurgeon, a psychiatrist, a family physician, a radiologist, and an interventional cardiologist may all carry the title “doctor,” yet the actual competencies required for excellence in these domains differ profoundly.
Despite this reality, many modern medical school admissions systems continue to operate under a generalized selection architecture that assumes one universal physician profile should be identified before specialization occurs.
This assumption increasingly deserves reconsideration.
The Problem pith the one-model approach
Current admissions systems in many Western countries heavily emphasize generalized holistic assessment:
- MMIs,
- CASPer,
- autobiographical narratives,
- communication-focused evaluation,
- behavioural interviews,
- and broad interpersonal assessment.
The justification is understandable:
modern healthcare requires professionalism, ethics, communication, and patient-centered care.
However, the same admissions architecture is used to select future:
- surgeons,
- pathologists,
- anesthesiologists,
- procedural specialists,
- technical diagnosticians,
- and highly analytical medical researchers.
This creates a structural mismatch.
Medicine contains multiple competency ecosystems, yet admissions systems often evaluate applicants through a single behavioural framework.
Different specialties require different strengths
A family physician requires:
- continuity of care,
- communication,
- emotional regulation,
- long-term patient management,
- and broad interpersonal engagement.
A surgeon requires:
- technical precision,
- visuospatial reasoning,
- rapid procedural decision-making,
- stress tolerance,
- endurance,
- and operational performance under pressure.
A radiologist depends heavily on:
- pattern recognition,
- analytical interpretation,
- and technical diagnostic cognition.
A pathologist may spend more time interpreting complex biological systems than interacting directly with patients.
Yet all are filtered initially through largely similar admissions structures.
This raises a critical institutional question:
Should one generalized admissions model determine entry into all future physician pathways?
Admissions Systems shape the profession
Admissions criteria are not neutral.
They shape:
- who applies,
- who succeeds,
- who self-selects out,
- and ultimately what kinds of physicians dominate the healthcare system.
If admissions systems heavily reward:
- behavioural presentation,
- interpersonal communication,
- empathy-oriented framing,
- and narrative performance,
then applicants strongest in those domains will increasingly dominate admission outcomes.
If systems emphasize:
- analytical rigor,
- scientific performance,
- technical reasoning,
- and procedural aptitude,
Different demographic and cognitive profiles may emerge because the architecture of selection determines the architecture of the profession itself.
The case for early differentiation
The future of medicine may require a more differentiated admissions model.
Instead of treating medicine as one homogeneous profession, admissions could eventually separate into partially specialized pathways earlier in the educational process.
For example:
|
Pathway |
Primary Competencies |
|
Surgery |
technical precision, stress tolerance, visuospatial reasoning |
|
Family Medicine |
communication, continuity of care, interpersonal management |
|
Radiology |
analytical interpretation, pattern recognition |
|
Psychiatry |
behavioural insight, emotional communication |
|
Research Medicine |
scientific reasoning, quantitative analysis |
Such a model would not eliminate shared medical foundations.
Rather, it would recognize that excellence across highly different medical domains may require different selection emphasis from the beginning.
Why the current model creates tension
One of the unintended consequences of generalized holistic admissions is that the system may disproportionately reward one behavioural archetype across all future specialties.
This can create several long-term effects:
- narrowing cognitive diversity,
- altering specialty pipelines,
- discouraging technically oriented applicants,
- reshaping workforce composition,
- and producing demographic outcomes strongly influenced by admissions architecture itself.
The paradox becomes especially visible in surgery.
Although women increasingly dominate medical school enrollment overall, surgery remains disproportionately male among practicing specialists. This suggests that medicine may not actually operate as one unified behavioural profession despite being selected through increasingly standardized behavioural criteria.
The profession diversifies later, even though the admissions system standardizes early.
The role of Technology and AI
This debate will intensify as medicine becomes more technologically integrated.
Future healthcare systems will increasingly involve:
- robotic surgery,
- AI-assisted diagnostics,
- precision medicine,
- advanced imaging systems,
- automated procedural support,
- and engineering-driven clinical environments.
Technical cognition may become even more important in several specialties.
In that environment, a universal admissions architecture centered primarily on generalized interpersonal screening may become progressively less aligned with the actual diversity of medical practice.
Communication still Matters but context matters more
None of this means communication should disappear from medicine.
Patients deserve:
- respect,
- informed consent,
- ethical treatment,
- and competent communication.
However, communication should not necessarily dominate admissions, weighting equally across every future specialty pathway.
A highly technical procedural specialist and a long-term community physician may require very different competency balances.
The admissions process should recognize this reality instead of assuming all future physicians should fit one standardized behavioural template.
Toward a more rational Admissions Architecture
A future-oriented admissions system may require:
- differentiated physician pathways,
- specialty-aligned competency weighting,
- stronger technical aptitude assessment for procedural fields,
- preserved interpersonal evaluation where clinically central,
- and earlier alignment between applicant strengths and future medical domains.
Medicine is not one profession anymore.
It is an ecosystem of highly differentiated technical, analytical, interpersonal, and procedural specialties operating under a shared ethical framework.
Admissions systems should evolve to reflect that reality.
Because the way a society selects physicians ultimately shapes the future structure, capability, and resilience of its healthcare system itself.
An article blog written with ChatGPT version. 5.5 support May 14, 2026
When you subscribe to the blog, we will send you an e-mail when there are new updates on the site so you wouldn't miss them.