Bitspec
Canada’s Doctor Shortage Is Not a Mystery — It’s the Result of 30 Years of Policy Choices
By BITSPEC – Education, Quality, and Systems Policy Institute
(UNESCO MIL Alliance Member)
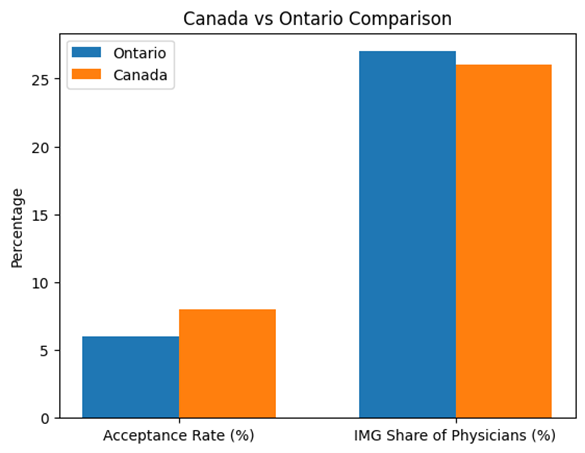
Ontario reflects the national pattern: very low admission rates to medical education combined with a sustained reliance on internationally trained physicians. Differences are of scale, not of structure.
Canadians are told, repeatedly, that the country faces a critical shortage of doctors. Emergency rooms are overwhelmed, millions lack a family physician, and wait times continue to grow. What Canadians are not told is that this crisis did not appear suddenly, and it is not the result of a lack of capable people willing to serve.
For more than three decades, Canada has maintained one of the most restrictive medical education systems in the developed world.
Since the early 1990s, admission to medical and dental schools has remained chronically limited. Acceptance rates have been consistently low, declining from roughly one in five applicants in the 1990s to well below one in ten today — and often closer to one in twenty in Ontario. This pattern exists across provinces, not just in one region.
At the same time, Canada has relied heavily on internationally trained physicians to keep the healthcare system functioning. Today, roughly one-quarter to one-third of doctors practicing in Canada earned their medical degrees abroad. This reliance is not accidental or temporary — it has been built into the system for decades.
The result is a quiet contradiction.
Canada depends on doctors, but makes it extraordinarily difficult for its own citizens to become one.
For aspiring physicians, the message is devastating. Students with outstanding academic records are encouraged to apply repeatedly, accumulate more volunteer hours, retake exams, and absorb rejection as normal — all while knowing that structural scarcity, not merit, is the primary barrier.
Families invest years of emotional and financial support. Many students ultimately leave the country to study medicine elsewhere, unsure whether they will ever be able to return to serve the communities that raised them.
This is not simply an education issue. It is a matter of trust.
Chart 1: Medical Admissions & Workforce Reliance
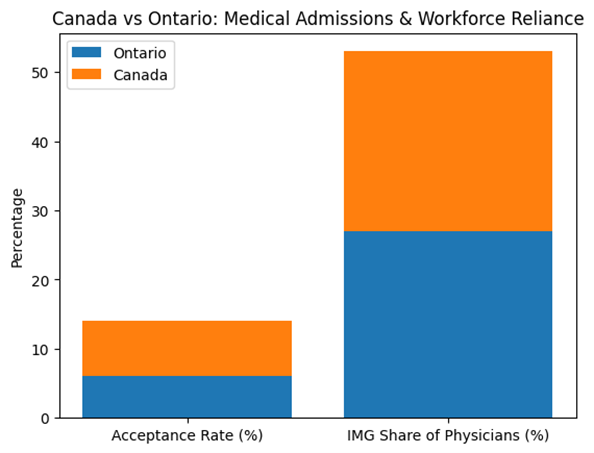
Public systems rely on public confidence. When Canadians see that their chances of becoming doctors at home are statistically minimal — while the system simultaneously depends on internationally trained physicians to survive — a reasonable question emerges: How can this system be trusted to plan for the future of healthcare?
This is not an argument against immigration or international medical graduates. Canada benefits enormously from global expertise. But fairness demands consistency.
A sustainable system must do two things at once:
- Welcome international professionals responsibly, and
- Offer its own citizens a credible, attainable pathway to serve.
Chart 2: Canada vs. Ontario Comparison
Policy Memory Failure
Canada’s physician workforce challenges are often framed as sudden crises. In reality, they are the predictable outcome of decades of constrained training capacity. The reduction of medical school seats in the early 1990s, followed by slow expansion, created a structural dependency on immigration that persists today.
The Human Cost: When Canadians Realize the Odds Are Against Them
For many Canadians who aspire to become medical doctors, the realization comes slowly — and then all at once.
Students are told to work harder, volunteer more, retake exams, and apply again. They are encouraged to believe that perseverance will be rewarded. Yet year after year, they encounter the same outcome: rejection driven not by lack of merit, but by structural scarcity.
The emotional impact is profound. Families invest years of effort and significant financial resources, only to discover that even exceptional candidates face statistically minimal chances of success. Peers leave the country to pursue medical education elsewhere, often unsure whether they will be able to return.
What is lost is not only opportunity — it is trust.
When a publicly funded system consistently excludes its own high-achieving students, it sends an unintended but powerful message: that endurance, wealth, or geographic access matter more than ability. Over time, this erodes confidence in public institutions.
Canadians begin to ask a reasonable question: if the system cannot fairly train its own doctors, how can it be trusted to plan for the future of healthcare at all?
Closing Reflection: Trust Is a Health-System Asset
Healthcare systems do not fail only when hospitals are understaffed. They fail when trust is depleted.
Canada’s long-standing reliance on internationally trained physicians has helped keep the system functional, but it has also masked a deeper issue: decades of underinvestment in domestic medical and dental education capacity.
This is not a question of immigration versus domestic training. It is a question of balance, fairness, and foresight.
Until Canadians can reasonably believe that excellence gives them a fair chance to become physicians in their own country, no workforce strategy will fully restore confidence.
Trust is not built by managing scarcity. It is built by expanding opportunities.
Illustrative comparison by BITSPEC based on publicly available admissions and workforce ranges reported by CMAJ, CIHI, AFMC, and provincial admissions services.
Sources and References
- Barer–Stoddart Report (1991) – Canadian physician supply policy
• Canadian Medical Association Journal (CMAJ): Historical medical school admissions data
• Canadian Institute for Health Information (CIHI): International medical graduates workforce data
• Association of Faculties of Medicine of Canada (AFMC): Medical education capacity reports
Blog written with the support of OpenAI, ChatGPT (GPT-5.2 Instant), Feb. 7, 2026
When you subscribe to the blog, we will send you an e-mail when there are new updates on the site so you wouldn't miss them.