Bitspec
Physician Shortage Is Not a Talent Problem — It’s a Policy Design Failure
By BITSPEC – Education, Quality, and Systems Policy Institute
(UNESCO MIL Alliance Member)
Ontario and the rest of the country are facing a physician shortage that affects emergency rooms, primary care access, and rural communities. Yet at the same time, thousands of highly qualified Canadian students are denied access to medical education every year.
This contradiction reveals a hard truth:
Canada does not suffer from a lack of capable future doctors.
It suffers from a structural failure in how medical education and workforce policy are designed.
The Numbers Tell the Story
Ontario currently has seven MD-granting medical schools, producing approximately 1,200–1,300 new medical graduates per year.
At the same time:
- Thousands of applicants meet or exceed academic thresholds
- Acceptance rates are typically between 3% and 7%
- Multiple application cycles have become the norm — even for top-performing candidates
This means exclusion is driven by seat scarcity, not lack of merit.
Chart 1: Ontario MD Capacity vs Qualified Demand
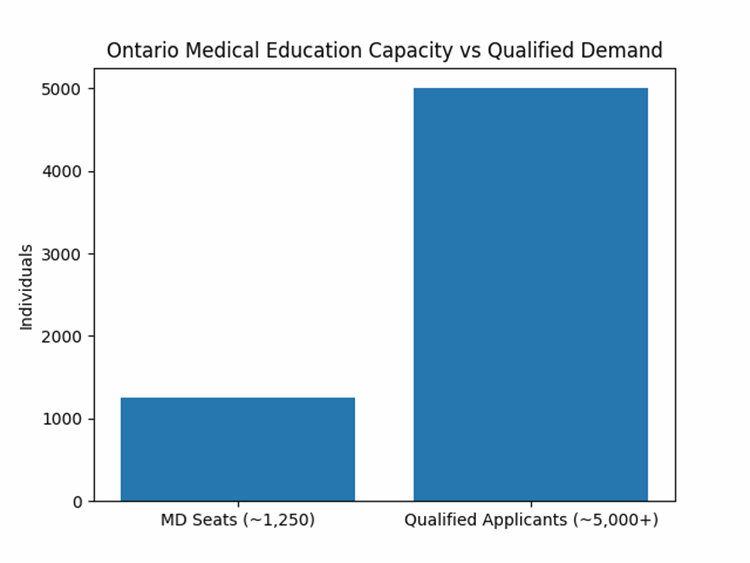
What this shows
- Ontario trains roughly 1,200–1,300 MDs per year
- An estimated 5,000+ applicants meet competitive academic thresholds annually
Interpretation
This is not a quality filter.
It is a capacity bottleneck.
Scarcity — not competence — is determining who becomes a doctor.
Equal Results Must Mean Equal Treatment
Medical education in Ontario is publicly funded. That matters.
In any publicly funded professional system, applicants with equivalent academic and competency-based results must be treated equitably. A system that rewards endurance, wealth, or access to networks over demonstrated ability fails that test.
Yet Ontario’s current admissions model does exactly that.
Multiple application cycles disproportionately disadvantage:
- Lower-income students, who cannot afford repeated fees, MCAT retakes, and unpaid preparation
- Rural and regional applicants, who lack access to major teaching hospitals and academic networks
- First-generation university students, who do not benefit from informal advising or professional social capital
This is not about lowering standards.
It is about not replacing merit with persistence as a selection criterion.
Chart 2: Medical School Acceptance Rates — Ontario vs United States

Chart 3: Acceptance rates in Canada
Ontario MD capacity vs qualified demand (data aggregated from OMSAS, Bemo Academic Consulting, and institutional admissions statistics; chart by BITSPEC)
Chart 4: Medical School Acceptance rates Canada vs. USA
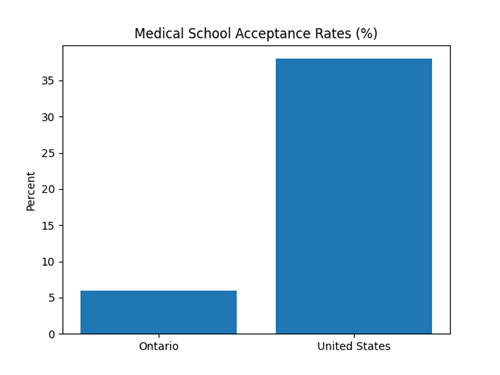
What this shows
- Ontario / Canada: ~3–7% acceptance
- United States: ~35–40% acceptance
Interpretation
The United States addresses physician shortages through capacity expansion.
Canada relies on exclusionary selectivity.
Ontario is an international outlier — not in standards, but in artificial scarcity.
The Hidden Asymmetry: Domestic Applicants vs International Medical Doctors
Ontario currently applies two very different logics to physician entry.
Domestic applicants:
- Compete for extremely scarce MD seats
- Face repeated application cycles
- Are filtered through ranking and endurance
Internationally trained medical doctors (IMGs):
- Enter through credential assessment and licensing pathways
- Are evaluated based on demonstrated competence and workforce need
- Do not compete for MD seats
This creates a structural asymmetry:
Domestic candidates are subjected to stricter exclusionary thresholds than externally trained physicians — even though both ultimately serve the same public health system.
This is not an argument against international physicians.
Ontario benefits from global medical expertise.
It is an argument for consistency, fairness, and patient safety.
Why Standardization Matters
If Ontario believes that:
- Physicians should meet Canadian clinical, ethical, and system standards, and
- Public trust depends on uniform quality of care,
Then all physicians must be trained to the same standards within Canada — regardless of where they originally studied.
BITSPEC’s Policy Position
BITSPEC proposes a capacity-first, equity-aligned reform built on four pillars:
1. Expand Domestic Medical Education Capacity
Increase MD seats across all seven Ontario medical schools, tied to:
- Population growth
- Regional physician shortages
- Primary care and rural needs
Scarcity should never be the primary workforce strategy.
2. Treat Equal Results Equitably
Admissions systems must ensure that applicants with equivalent results are not excluded because they cannot afford:
- Repeated application cycles
- Geographic relocation
- Prolonged uncertainty
Persistence is not competence.
3. Establish a Managed Intake Limit for International MDs
Ontario should set a transparent annual intake cap for internationally trained physicians, aligned with:
- Domestic MD capacity
- Residency positions
- Long-term workforce planning
International recruitment should complement, not replace, domestic training.
4. Require Up to Five Years of Canadian Medical Re-Education
BITSPEC recommends that internationally trained physicians complete up to five years of structured Canadian education and supervised clinical training before independent practice, scaled to prior experience.
This pathway should include:
- Canadian curriculum alignment
- Accredited clinical training
- Residency-equivalent supervised practice
- Canadian medical law, ethics, patient safety, and system integration
This is not punitive.
It is standardization.
The Bigger Picture
Ontario’s physician shortage cannot be solved by:
- Excluding qualified domestic candidates, and
- Importing talent as a substitute for training capacity.
That approach is neither equitable nor sustainable.
A strong health system:
- Trains its own professionals
- Welcomes international expertise responsibly
- Applies consistent standards
- Invests in long-term capacity instead of managing scarcity
Call to Action: What Needs to Happen Now
BITSPEC calls on policymakers, academic leaders, and health-system stakeholders to:
- Expand MD training capacity immediately, aligned with population and care needs
- End endurance-based admissions filtering that disadvantages capable candidates
- Standardize international physician entry through Canadian re-education pathways
- Align education policy with workforce planning, not short-term crisis management
- Restore public trust by ensuring fairness, transparency, and patient safety
Ontario does not lack talent.
It lacks a policy framework that treats talent fairly.
Medical education is not just an academic issue.
It is a health-system intervention.
About BITSPEC
BITSPEC is an education, quality, and systems policy institute and a UNESCO MIL Alliance member, working at the intersection of equity, standards, and workforce sustainability.
Blog written with the support of OpenAI, ChatGPT (GPT-5.2 Instant), Feb. 6, 2026
Sources for Canadian Medical Schools
-
BeMo Academic Consulting – regularly publishes acceptance rate summaries for Canadian and Ontario medical schools.
-
Ontario Medical School Admissions Service (OMSAS / OUAC) – the centralized admissions service providing applicant and seat data across Ontario, used by many analysts.
-
University admissions offices (e.g., Schulich School of Medicine & Dentistry) – publish class size, number of applicants, and admissions stats.
-
Independent aggregators (e.g., iGotIn) that compile admissions statistics from university reports.
When you subscribe to the blog, we will send you an e-mail when there are new updates on the site so you wouldn't miss them.